November 14 marks World Diabetes Day, a global effort to raise awareness about the growing impact of diabetes, prevention strategies, and the latest advancements in diabetes care. At Burjeel Hospital, our endocrinology team is dedicated to empowering our community with essential knowledge and resources for managing and preventing diabetes.
Understanding Diabetes
Diabetes is a chronic condition affecting how the body processes blood glucose (sugar). There are two main types of diabetes:
Type 1 Diabetes: An autoimmune condition in which the body attacks insulin-producing cells in the pancreas, often diagnosed in younger people.
Type 2 Diabetes: The most common form, often linked to lifestyle factors like diet, exercise, and genetics, primarily affecting adults but increasingly seen in children and adolescents.
Why Is World Diabetes Day Important?
Diabetes continues to impact millions of lives worldwide, with rising cases of type 2 diabetes driven by lifestyle changes and urbanization. World Diabetes Day serves as a reminder to stay informed and proactive in managing health risks.
Expert Tips from Our Endocrinologists
At Burjeel, our endocrinologists recommend the following lifestyle practices to help prevent or manage diabetes effectively:
Healthy Eating Habits: A balanced diet rich in whole grains, lean proteins, fruits, and vegetables helps manage blood sugar levels and maintain a healthy weight. Minimizing sugary foods and refined carbs is crucial.
Regular Physical Activity: Engaging in daily physical activities like walking, jogging, or swimming can improve insulin sensitivity, reduce body fat, and support overall well-being.
Routine Checkups and Monitoring: Regular checkups, including blood glucose and HbA1c testing, can help monitor blood sugar levels and detect any warning signs early.
Stress Management: Chronic stress can raise blood glucose levels, especially in individuals with diabetes. Mindfulness practices like meditation, deep breathing, and hobbies can be helpful.
Awareness of Symptoms: For early detection, it’s essential to recognize symptoms like frequent urination, excessive thirst, fatigue, and unexplained weight loss, which can be signs of diabetes.
Advancements in Diabetes Care at Burjeel
Our endocrinology department offers cutting-edge treatments and personalized care plans, including:
Continuous Glucose Monitoring (CGM): CGM devices help track blood sugar levels in real-time, allowing for better management.
Insulin Therapy: We provide advanced insulin therapies tailored to individual needs.
Diabetes Education Programs: Our patient education sessions cover lifestyle guidance, dietary advice, and medication management for sustainable diabetes care.
Join Us in Raising Awareness
On this World Diabetes Day, join Burjeel Hospital in spreading awareness and encouraging healthy practices that can reduce the burden of diabetes on individuals and families. Small steps today can lead to a healthier tomorrow.
As we age, our bodies undergo numerous changes, many of which can affect our bones. One of the most common conditions affecting bone health is osteoporosis—a silent disease that weakens bones, making them more prone to fractures. While osteoporosis can affect anyone, it is more prevalent among postmenopausal women, elderly individuals, and people with certain medical conditions.
What Is Osteoporosis?
Osteoporosis is a condition that results in weakened bones, increasing the risk of fractures, especially in the hips, spine, and wrists. The word “osteoporosis” literally means “porous bone,” which reflects the loss of bone density and strength over time. This condition occurs when the creation of new bone doesn’t keep up with the removal of old bone, leading to a fragile skeletal structure.
Causes and Risk Factors
Several factors can contribute to the development of osteoporosis, including:
Age: Bone mass naturally decreases as we age, with most people reaching peak bone mass in their late 20s. After this, bone density gradually declines.
Hormonal Changes: Women are at a higher risk of osteoporosis, especially after menopause when estrogen levels drop significantly. Estrogen is essential for maintaining bone density. Similarly, men with reduced testosterone levels may also face an increased risk.
Genetics: A family history of osteoporosis or fractures may predispose you to developing the condition.
Dietary Deficiencies: A lack of calcium and vitamin D weakens bones, making them more vulnerable to osteoporosis.
Lifestyle Factors: Smoking, excessive alcohol consumption, a sedentary lifestyle, and a lack of weight-bearing exercises can contribute to bone loss.
Medical Conditions and Medications: Certain conditions, such as thyroid problems, rheumatoid arthritis, or malabsorption syndromes, and medications like corticosteroids, can increase the risk of osteoporosis.
Symptoms of Osteoporosis
Osteoporosis is often called the “silent disease” because most people are unaware they have it until they experience a fracture. However, there are some signs to watch for:
Back pain: This can be caused by a fracture or collapsed vertebra.
Loss of height over time: Gradual loss of height can be an indication of osteoporosis-related vertebral compression fractures.
Stooped posture: Known as kyphosis, this can result from the weakening of the spine.
Fractures: Even minor falls or simple actions, such as bending over or coughing, can lead to fractures in people with severe osteoporosis.
Diagnosis and Testing
Osteoporosis is diagnosed through a bone density test, typically a dual-energy X-ray absorptiometry (DEXA) scan. This test measures the density of bones in your spine, hip, and other areas to assess your fracture risk.
Preventing Osteoporosis: Steps for Stronger Bones
While osteoporosis may not be entirely preventable, there are several steps you can take to protect your bones and reduce your risk:
Calcium-Rich Diet: Ensure you’re getting enough calcium through dairy products, leafy greens, and fortified foods. Calcium is essential for maintaining strong bones.
Vitamin D: Vitamin D helps your body absorb calcium. You can obtain it from sunlight, fortified foods, or supplements.
Exercise Regularly: Weight-bearing exercises, such as walking, jogging, and strength training, help build and maintain bone density. Exercises like yoga and Pilates improve balance, reducing the risk of falls.
Avoid Smoking and Excessive Alcohol: Smoking and drinking alcohol excessively can weaken bones, so it’s important to avoid these habits to protect your bone health.
Bone-Strengthening Medications: If you are at high risk of fractures, your doctor may prescribe medications to help slow bone loss and rebuild bone density.
Routine Screenings: If you are over 50 or have risk factors for osteoporosis, routine bone density screenings are crucial. Early detection allows for better management of the condition.
Managing Osteoporosis
If you have been diagnosed with osteoporosis, don’t lose hope. There are effective treatments available. Medications such as bisphosphonates, selective estrogen receptor modulators (SERMs), and hormone replacement therapy (HRT) can slow bone loss and reduce the risk of fractures. Your endocrinologist will help create a tailored plan to protect your bones and prevent further complications.
Conclusion
Osteoporosis is a serious but manageable condition. By adopting healthy lifestyle habits, staying informed about your bone health, and seeking early intervention, you can significantly reduce your risk of osteoporosis and maintain strong bones for life.
At Burjeel Hospital, we are committed to helping you achieve optimal health and wellness. If you are concerned about your bone health or want to learn more about osteoporosis, we encourage you to schedule a consultation with one of our specialists. Together, we can help you build stronger bones and lead a healthier, more active life.
You must carefully read the “Consumer Information Use and Disclaimer” below in order to understand and correctly use this information.
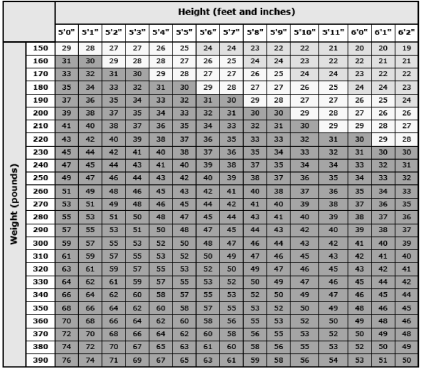
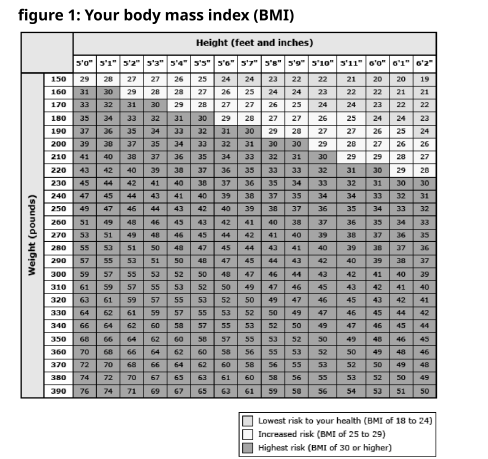
What is obesity? Doctors define obesity based on a person’s “body mass index,” or “BMI.” For adults, weight and height are used to calculate BMI (figure 1). For people who are White, Hispanic, or Black: ● “Overweight” means a BMI between 25 and 29.9. ● “Obesity” means a BMI of 30 or greater. For people who are Asian, the cutoff numbers are a little different: ● “Overweight” means a BMI between 23 and 25. ● “Obesity” means a BMI of 25 or greater. In addition to figuring out your BMI, your doctor might also measure around your belly. This is called “waist circumference.” Doctors call it “central obesity” when people carry extra weight in the belly area, even if their BMI is normal. Obesity increases the risks of many different health problems. It can also make it harder for you to move, breathe, and do other activities. What are the health risks of obesity? — Having obesity increases a person’s risk of developing many health problems. Here are just a few examples: ● Diabetes ● High blood pressure ● High cholesterol ● Heart disease (including heart attacks) ● Stroke ● Sleep apnea (a disorder that makes you stop breathing for short periods while asleep) ● Asthma ● Cancer 18/09/2024, 11:28 Patient Education – UpToDate® Lexidrug™ https://online.lexi.com/lco/action/pcm 1/4
Does having obesity shorten a person’s life? — Yes. Studies show that: ● People with obesity die younger than people who are a healthy weight. ● The risk of death goes up the heavier a person is. The degree of increased risk depends on how long the person has had obesity, and on what other medical problems they have.
People with central obesity (extra weight in the belly area) might also be at risk of dying younger.
Can medical treatments help me lose weight? —
Yes. There are medicines and surgery to help with weight loss. These treatments are meant for people who have not been able to lose weight through lifestyle changes such as diet and exercise. Weight loss treatments do not take the place of diet and exercise. People who have the treatments must also change how they eat and how active they are. How can I prevent the problems caused by obesity? — The best thing you can do is lose weight. But even if weight loss is not possible, you can improve your health and lower your risk if you: ● Become more active – Many types of physical activity can help, including walking. You can start with a few minutes a day, and add more as you get stronger and build up your endurance. Anything that gets your body moving is good for you. It is easier to create a habit if you choose activities you enjoy. ● Improve your diet – It is healthy to have regular meal times, eat smaller portions, and not skip meals. Limit sweets, and avoid processed foods. Try to eat more vegetables and fruits instead. The best weight loss plans help you have a healthy view of eating. ● Quit smoking (if you smoke) – Some people start eating more after they stop smoking, so try to make healthy food choices. Even if it increases your appetite, quitting smoking is still one of the best things you can do to improve your health. ● Limit alcohol – For females of any age, limit alcohol to no more than 1 drink a day. For males 64 and younger, limit alcohol to no more than 2 drinks a day. For males 65 and older, limit alcohol to no more than 1 drink a day. Keeping a diary might help you reach your daily goals. You can use a paper diary or app to help you record: ● What you eat and drink ● Your physical activity ● Your weight
What causes obesity? — Your genes affect your risk of obesity. But lifestyle also has a big impact. You can develop obesity if you eat too much, eat unhealthy foods, move too little, and watch a lot of TV.
There are other things that seem to increase the risk of obesity that you might not know about. Here are some: ● Mother’s habits during and after pregnancy – People who eat a lot of calories, have diabetes, or smoke during pregnancy have a higher chance of having babies who have obesity as adults. Also, babies who drink formula might be more likely than breastfed babies to develop obesity later in life. ● Habits and weight gain during childhood – Children or teens who are overweight or have obesity are more likely to have obesity as an adult. ● Sleeping too little – People who do not get enough sleep are more likely to develop obesity. ● Taking certain medicines – Long-term use of certain medicines can cause weight gain. If you are concerned that one of your medicines might be making you gain weight, talk to your doctor or nurse. They might be able to switch you to a different medicine. ● Certain hormonal conditions – Some hormonal problems can increase the risk of developing obesity. For example, hypothyroidism can cause weight gain, along with other symptoms.
What if I want to get pregnant? — If you are overweight or have obesity, it might be harder to get pregnant. For males, obesity can also cause sex problems, like having trouble getting or keeping an erection. This is more likely if you also have high blood pressure or diabetes. What if my child has obesity? — In children, obesity has many of the same risks as it does in adults. For example, it can increase the risk of diabetes, high blood pressure, asthma, and sleep apnea. It can also cause added problems related to childhood. For example, obesity can make children grow faster than normal and cause girls to go through puberty earlier than usual. When should I call the doctor? — Call your doctor or nurse if you want to try to lose weight. They can help you do it in a healthy way. It can also help to work with a dietitian (food and nutrition expert). They can help you choose healthy foods and plan meals. All topics are updated as new evidence becomes available and our peer review process is complete. This topic retrieved from UpToDate on: Jul 13, 2024.
Find your height (in feet and inches) in the top row. Then, find your weight (in pounds) in the first column. Now, find where the column for your height and the row for your weight meet. That is your BMI. For example, if you are 5-feet-9-inches tall and you weigh 260 pounds, your BMI is 38. Graphic 62886 Version 4.0 Consumer Information Use and Disclaimer:
Breast cancer is one of the most common cancers affecting women globally. The good news is that when detected early, it can be treated successfully. Early detection plays a vital role in improving survival rates, which is why it’s important for every woman to know the signs and symptoms of breast cancer and stay vigilant about her breast health.
Why Early Detection Matters
Breast cancer doesn’t usually cause pain or noticeable symptoms in its earliest stages, making regular screening and awareness crucial. When caught early, breast cancer treatment is often more effective and less invasive, with higher survival rates. That’s why self-awareness and routine medical checkups are key to catching breast cancer before it spreads.
Early Symptoms of Breast Cancer to Watch For
Breast cancer can present itself in a variety of ways. It’s important to know your body and recognize changes. Here are some common signs that may indicate early breast cancer:
1. Lump or Mass in the Breast: One of the most common symptoms of breast cancer is the presence of a lump or mass in the breast. This mass is often hard and painless, but in some cases, it can feel tender or soft. Not all lumps are cancerous, but if you find one, it’s critical to consult your doctor for further evaluation.
2. Changes in Breast Size or Shape: Noticeable changes in the size or shape of one breast compared to the other can be an early indicator of breast cancer. Sudden swelling, shrinkage, or asymmetry should not be ignored.
3. Skin Changes on the Breast: Breast cancer can sometimes cause changes to the skin covering the breast, including:
Dimpling or a texture resembling an orange peel.
Redness or a rash that doesn’t go away.
Thickening or swelling in the breast. These changes may be subtle, but they’re important to discuss with your healthcare provider.
4. Nipple Changes: Nipple changes are another potential warning sign of breast cancer. Keep an eye out for:
Inverted or retracted nipples (when the nipple turns inward).
Discharge from the nipple, especially if it’s bloody or occurs without squeezing.
Scaling, peeling, or flaking skin around the nipple. While some nipple changes can be linked to hormonal shifts, they could also signal underlying issues like breast cancer.
5. Unexplained Breast Pain: While breast pain is more commonly associated with hormonal changes, persistent or unusual pain in one area of the breast that doesn’t go away with your menstrual cycle could be a sign of something more serious.
6. Lumps in the Armpit: Breast cancer can spread to nearby lymph nodes, including those in the armpit area. If you notice any unusual swelling or lumps in your armpit, it’s important to bring this to your doctor’s attention.
How to Detect Breast Cancer Early
There are several steps you can take to ensure breast cancer is detected at its earliest and most treatable stage:
1. Perform Regular Breast Self-Exams Knowing what’s normal for your breasts can help you detect changes early. A breast self-exam should be done monthly, ideally a few days after your period ends. Here’s how to perform a self-exam:
In front of a mirror, inspect your breasts with your arms at your sides and then raised overhead. Look for changes in size, shape, and skin texture.
Lying down, use the pads of your fingers to feel your breasts in circular motions, checking the entire breast, armpit, and collarbone area.
In the shower, feel for any lumps or changes with soapy hands, which can help detect subtle differences. If you notice any changes, make an appointment with your doctor for further evaluation.
2. Get Regular Mammograms Mammograms are the most reliable method for detecting breast cancer in its early stages. Most women should start having mammograms at age 40, but if you have a family history of breast cancer or other risk factors, your doctor may recommend starting earlier. Mammograms can detect tumors before they’re large enough to feel and can identify abnormal areas that need further investigation. Make sure to schedule a mammogram as part of your regular health check-up.
3. Clinical Breast Exams In addition to self-exams and mammograms, your OB-GYN or primary care physician should perform a clinical breast exam during your annual check-up. This is an important opportunity to discuss any changes you’ve noticed and receive a professional evaluation.
4. Genetic Testing for High-Risk Women Women with a family history of breast cancer may benefit from genetic testing to determine if they carry BRCA1 or BRCA2 gene mutations, which increase the risk of breast and ovarian cancers. If you’re identified as high-risk, your doctor may recommend more frequent screenings or preventive measures.
Reducing Your Risk of Breast Cancer
While some risk factors for breast cancer, such as age and family history, are out of your control, there are several lifestyle choices you can make to reduce your risk:
Maintain a healthy weight: Obesity, especially after menopause, has been linked to an increased risk of breast cancer.
Exercise regularly: Staying active helps maintain a healthy weight and lowers your risk.
Limit alcohol consumption: Excessive alcohol intake is associated with a higher risk of breast cancer.
Breastfeed: Breastfeeding has been shown to lower the risk of developing breast cancer, especially in women who breastfeed for over a year.
Avoid smoking: Smoking has been linked to many types of cancer, including breast cancer.
Conclusion: Stay Vigilant and Informed
Early detection of breast cancer is critical for successful treatment, and staying informed about the early warning signs can make all the difference. Be proactive about your breast health—perform regular self-exams, schedule routine mammograms, and maintain a healthy lifestyle. At Burjeel Hospital, our team of experts is dedicated to providing comprehensive care for women. If you have concerns about your breast health or want to schedule a screening, our experienced doctors are here to guide you through the process with compassion and expertise.
This website uses cookies. We use cookies to make sure you get the best experience on our website. Please read our privacy policy and Terms & Conditions.
Burjeel Holdings Cookie Policy
Our website uses cookies and similar tracking technologies to enhance website functionality and analyze site usage. Our aim is to improve the experience for visitors to our website.
What is a cookie?
Cookies are small text files downloaded to your device when you visit a website. Cookies are also sent back to the original website or another website that recognises the cookie and act as a memory for a website, allowing the site to remember details on subsequent visits. For instance, cookies can remember end user preferences, improve user experience as well as adjust content to items most relevant to end users
Burjeel Holdings uses cookies for the following purposes:
Providing website functionality;
Analyzing site usage
Generic type cookies
Session and persistent cookies
When a site is launched, these cookies attempt to remember information about you, such as your consent to view YouTube videos or to use investor tools
Session cookies exist only until you close your web browser
Persistent cookies exist longer but for a specified period of time.
Third party cookies
Third-party cookies are created by domains that are not the website (or domain) that you are visiting. These cookies are used to understand your browsing of the website, for example, which page you visit or how long you stay on each page.
These types of cookies are set by Burjeel Holdings affiliates and/or vendors we are working with to enhance end user experience
The Cookie Preferences Panel
You may utilize the Cookie Preferences Panel at any time to change or withdraw your consent for each cookie category - except strictly necessary cookies - by clicking the “Cookie preferences” button in the bottom of the screen or clicking the “Cookie Policy“ link, located in the website footer. You may select “Allow all cookies” on the panel which permits the download of all available cookies for use.
The panel identifies categories of cookies and enables you to control and change your cookie preferences. Detailed information about the individual cookies is provided on Cookie Policy page, it is delivered in an open and transparent way, providing complete visibility into how cookies are used to enrich your visitor experience and make an informed choice to allow their usage.
You may use the Toggle bar next to each category of cookies to set acceptance or denial of cookies being placed on your device. Be aware however, that restricting cookies may impact the functionality of a website. Many of the interactive functions offered by websites are dependent on cookies and disabling or blocking cookies can prevent these services from working and reduce their usefulness. Once your selections are made, click the “Confirm your preferences” button to confirm your cookie usage choices.
Cookie Category Description
Mandatory Cookies
The strictly necessary cookies help make a website usable by enabling basic functions like page navigation and access to secure areas of the website. These cookies are necessary for the website to function and cannot be switched off in our systems. They are usually only set in response to actions made by you which amount to a request for services, such as setting your privacy preferences, logging in or filling in forms. You may be able to decline these cookies through your browser, but necessary parts of the site will not then work. These cookies do not store any personally identifiable information.
Operational Cookies
These cookies allow us to count visits and traffic sources, perform customer surveys and other web analytics, so we can measure and improve the performance of our site. They help us know which pages are the most and least popular and see how visitors move around the site. The information these cookies collect is aggregated and in some instances limited identifiable data may be collected.
Functional Cookies
These cookies enable the website to provide enhanced functionality, aid site personalisation, maintain user-selected options and site navigation aids. They may be set by us or by third party providers whose services we have added to our pages. If you do not allow these cookies then some or all of these services may not function properly.
Marketing and targeted advertising cookies
They are not used on this website.
Individual Cookies Descriptions
You can find more information about the individual cookies we use and the purposes for which we use them in the table below:
Name
Provider
Purpose
Expiry
Type
Operational
_ga
Google
Registers a unique ID that is used to generate statistical data on how the visitor uses the website.
2 years
HTTP Cookie
_ga_#
Google
Used by Google Analytics to collect data on the number of times a user has visited the website as well as dates for the first and most recent visit.
2 years
HTTP Cookie
Functional
cookies_policy
Burjeel Holdings
Stores the user’s cookie consent state for the current domain.
1 year
HTTP Cookie
SERVERID
Closir
Session
HTTP Cookie
_hjSessionUser_#
Closir
1 year
HTTP Cookie
_hjSession_#
Closir
1 day
HTTP Cookie
CLID
Euroland
351 day
HTTP Cookie
MUID
Euroland
371 day
HTTP Cookie
Marketing
VISITOR_INFO1_LIVE
YouTube
Tries to estimate the users’ bandwidth on pages with integrated YouTube videos.
180 days
HTTP Cookie
YSC
YouTube
Registers a unique ID to keep statistics of what videos from YouTube the user has seen.
Session
HTTP Cookie
We only use necessary cookies that help make a website usable by enabling basic functions like page navigation and access to secure areas of the website. The website cannot function properly without these cookies.We and do not store any PII data on the websites.
Azure Cookies
Azure TuPMix
Description : The TiPMix cookie is set by Azure to determine which web server the users must be directed to.
Duration : 1 hour
Azure x-ms-routing-name
Description : Azure sets this cookie for routing production traffic by specifying the production slot.
Duration : 1 hour
Azure ARRAfinity
Description : ARRAffinity cookie is set by Azure app service, and allows the service to choose the right instance established by a user to deliver subsequent requests made by that user.
Duration : Session
Azure ARRAffinitySamSite
Description : This cookie is set by Windows Azure cloud, and is used for load balancing to make sure the visitor page requests are routed to the same server in any browsing session
Duration : Session
Analytics cookies
Google Tag Manager _gcl_au
Description : Google Tag Manager sets the cookie to experiment advertisement efficiency of websites using their services.
Duration : 3 months
Google Analytics _ga_*
Description : Google Analytics sets this cookie to store and count page views.
Duration : 1 year 1 month 4 days
Google Analytics _ga
Description : Google Analytics sets this cookie to calculate visitor, session and campaign data and track site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognise unique visitors.
Duration : 1 year 1 month 4 days
Google Analytics ga*
Description : Google Analytics sets this cookie to store and count page views.
Duration : 1 year 1 month 4 days
Facebook _fbp
Description : Facebook sets this cookie to display advertisements when either on Facebook or on a digital platform powered by Facebook advertising after visiting the website.
Duration : 3 months
Functional Cookies
Polylang pll_language
Description : These are used to remember the language the user selects when returning to the website and get the language information when unavailable in another way.
Duration : 1 year
We are currently using only the mandatory cookies, and the websites cannot function properly without these. None of the cookies are storing any user data [like -- login information, items in shopping cart, users tracking for advertising purposes, user preferences and activities].
Along with the Cookie Preferences Panel, you can also change your browser and/or mobile device settings so that cookies from this website cannot be placed on your computer or mobile device. You can usually change the browser’s settings to refuse new cookies, disable existing ones or simply let you know when new ones are sent to your device. In order to set your browser to reject cookies, refer to the help instructions supplied by the browser provider (usually located within the “Help”, “Tools” or “Edit” menu) or the settings of your mobile device.
Please be aware that, if you refuse or disable cookies, some of the website’s functionality may be lost.
Learn more about who we are, how you can contact us and how we process personal data in our Privacy Policy If you have any queries in relation to this notice, please contact us at dataprotectionofficer@burjeelholdings.com