Understanding an Exceptionally Rare Urological Anomaly
Retrocaval ureter, also known as circumcaval ureter or preureteral vena cava, represents one of the rarest congenital anomalies in urological practice. With an estimated incidence of just 0.06-0.17% worldwide, this condition presents a unique diagnostic and surgical challenge for urologists. A recent case successfully managed at Burjeel Hospital highlights both the complexity and optimal management approaches for this unusual condition.
The Embryological Puzzle
Despite its name suggesting a ureteral anomaly, retrocaval ureter actually results from an abnormal development of the inferior vena cava (IVC) during embryological development. The condition occurs when the right ureter becomes entrapped behind the IVC, coursing posteriorly and then medially around the vein before resuming its normal position distally. This creates the characteristic “fishhook” or “reverse J” deformity visible on imaging studies.
Interestingly, while the anomaly is present from birth, symptoms typically don’t manifest until the third or fourth decade of life, when progressive obstruction leads to clinical presentations.
Clinical Presentation: A Diagnostic Challenge
The patient in this case presented with a classic constellation of symptoms that characterize retrocaval ureter:
- Intermittent right flank pain persisting for several months
- Episodes of urinary tract infections
- Nonspecific symptoms that had previously led to misdiagnosis
What makes this condition particularly challenging from a diagnostic perspective is its similarity to more common conditions like urolithiasis (kidney stones). Patients often undergo multiple evaluations and treatments for suspected stones before the correct diagnosis is established.
Advanced Imaging: The Key to Diagnosis
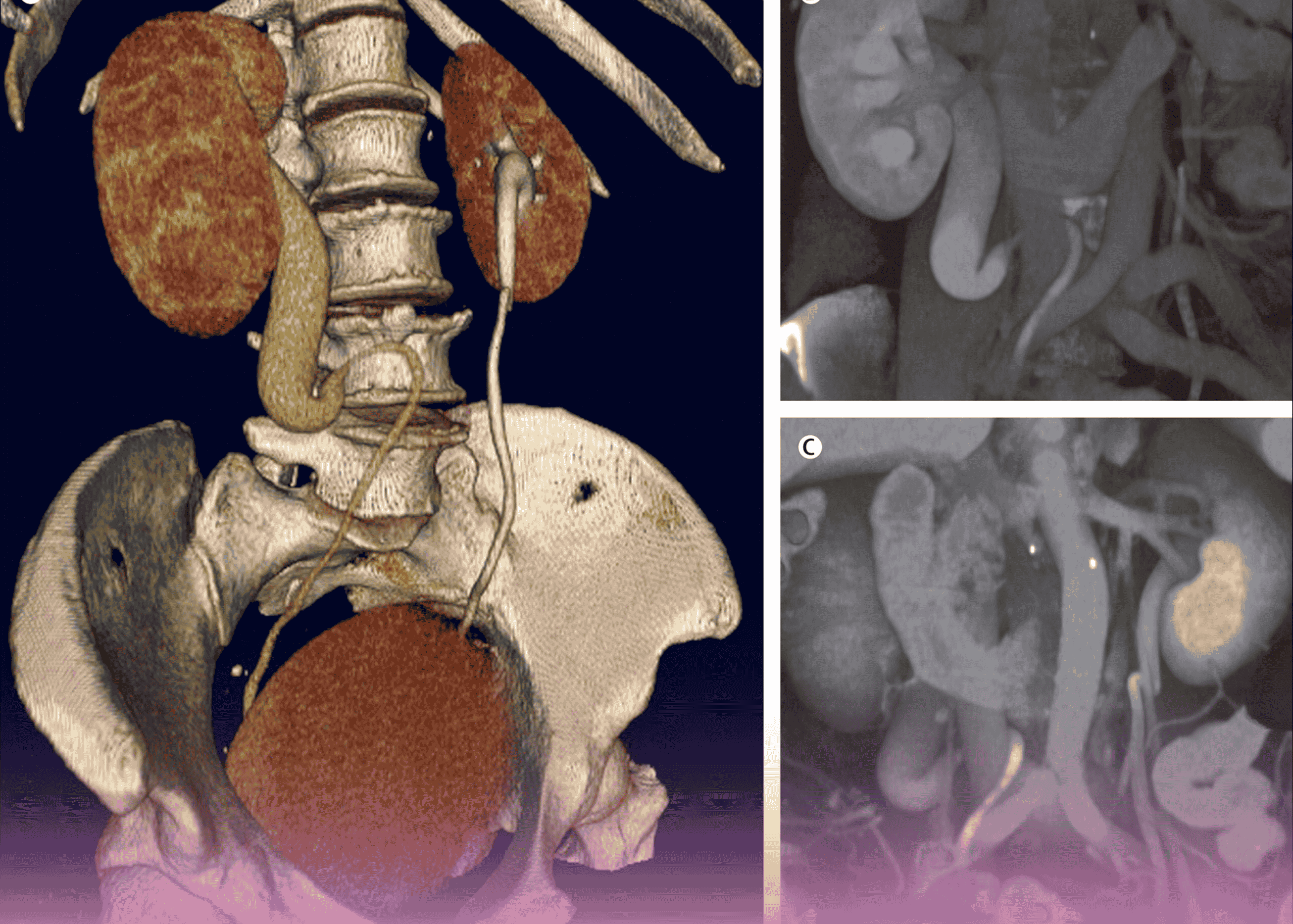
The definitive diagnosis in this case was established through contrast-enhanced CT urography, which revealed the pathognomonic findings of:
- Right-sided hydronephrosis (dilation of the kidney collecting system)
- Hydroureter proximal to the retrocaval segment
- The classic “fishhook” or “S-shaped” appearance of the proximal ureter as it courses behind the IVC
- Normal caliber of the distal ureter after emerging from behind the IVC
This case highlights the critical importance of appropriate imaging studies in the diagnosis of rare urological conditions. While ultrasound may detect hydronephrosis, CT urography with multiplanar reconstruction provides the detailed anatomical information necessary for surgical planning.
Surgical Approach: Precision and Expertise
The surgical management of retrocaval ureter has evolved significantly over recent decades. In this case, the surgical team employed a carefully planned approach that included:
- Preoperative stenting: Placement of a double-J ureteral stent to maintain drainage and facilitate identification during surgery
- Transperitoneal approach: Providing excellent exposure of both the ureter and the IVC
- Careful ureteral dissection: Identifying the point of obstruction where the ureter passes behind the IVC
- Resection of the retrocaval segment: Removing the narrowed, often aperistaltic portion of ureter trapped behind the IVC
- Ureteroureteral anastomosis: Precise reconnection of the ureter anterior to the IVC, positioning it in its anatomically correct location
- Stent placement: Ensuring proper healing and drainage during the recovery period
While traditionally performed as an open procedure, advances in minimally invasive surgery have made laparoscopic repair increasingly common, offering benefits of reduced postoperative pain, shorter hospital stay, and improved cosmetic results. The surgical team’s expertise allowed for a successful outcome despite the technical challenges inherent in this rare condition.
Postoperative Care and Outcomes
Following surgery, the patient’s recovery was monitored with particular attention to:
- Urinary output and drain output
- Resolution of preoperative pain
- Follow-up imaging to confirm resolution of hydronephrosis
- Eventual removal of the ureteral stent after ensuring proper healing
The patient experienced complete resolution of symptoms following surgery, with follow-up imaging demonstrating significant improvement in the previously dilated collecting system. This successful outcome illustrates the importance of proper diagnosis and definitive surgical correction for symptomatic retrocaval ureter.
Clinical Significance and Learning Points
This case highlights several important clinical lessons:
- Consider rare anomalies: When evaluating patients with recurrent right flank pain and hydronephrosis without obvious stone disease, rare anatomical variations should be considered.
- Value of cross-sectional imaging: CT urography provides detailed anatomical information critical for diagnosing vascular anomalies affecting the urinary tract.
- Timing of intervention: While the anomaly is congenital, intervention is typically only required when symptoms develop, usually in adulthood.
- Multidisciplinary approach: Collaboration between urologists, radiologists, and surgical teams ensures optimal outcomes for these complex cases.
Conclusion
Retrocaval ureter represents a fascinating intersection of embryological development, anatomical variation, and surgical expertise. While rare, this condition serves as an important reminder of the value of thorough diagnostic evaluation and the need to consider uncommon etiologies when common explanations fail to account for a patient’s symptoms.
The successful management of this case at Burjeel Hospital demonstrates the institution’s capability in handling complex urological anomalies, providing patients with access to advanced diagnostic and surgical care for even the rarest of conditions.

