Introduction
Complex Regional Pain Syndrome (CRPS) represents one of the most challenging pain conditions to manage effectively. Characterized by intense pain disproportionate to the inciting event, along with autonomic, sensory, and motor abnormalities, CRPS can be severely debilitating for patients. This case study explores the successful implementation of lumbar sympathetic block as an interventional pain management technique for CRPS following knee surgery, highlighting its efficacy in providing relief when conservative treatments fail.
Understanding Lumbar Sympathetic Block
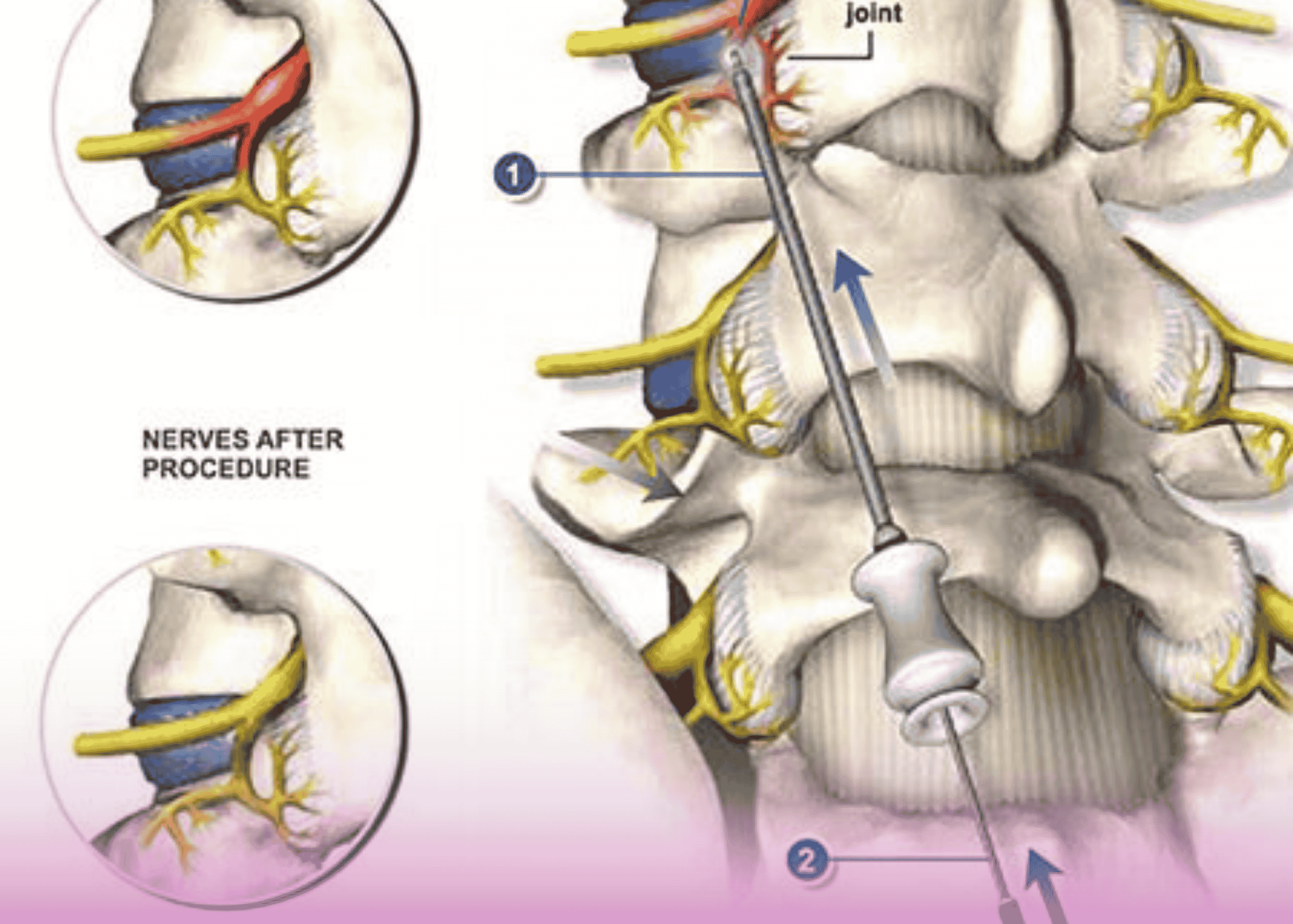
A lumbar sympathetic block is a minimally invasive pain management procedure designed to disrupt the nerve supply from the sympathetic chain to the lower extremities. This intervention targets the sympathetic nervous system, which plays a critical role in pain perception and transmission, particularly in conditions with sympathetically maintained pain components.
Anatomical Considerations
The lumbar sympathetic ganglia form a chain of nerve cell bodies that run parallel to the vertebral column in the retroperitoneal space. The densest portion of these ganglia is typically found at the L2 and L3 vertebral levels, making these the optimal targets for intervention. The procedure is most commonly performed at the L3 level, providing effective disruption of sympathetic innervation to the lower limbs.
Procedural Approach
The lumbar sympathetic block procedure typically follows a two-step approach:
- Diagnostic Block: Initially, a diagnostic block using only local anesthetic is administered to assess the patient’s response. This serves as a predictor of success for more definitive interventions.
- Therapeutic Intervention: If optimal relief is achieved with the diagnostic block, radiofrequency ablation is subsequently performed at the L2, L3, and L4 levels to provide longer-lasting relief.
Primary Indications
Lumbar sympathetic blocks are primarily indicated for several painful conditions affecting the lower extremities:
- Complex Regional Pain Syndrome (CRPS)
- Phantom limb pain
- Hyperhidrosis (excessive sweating)
- Vascular insufficiencies
- Herpes zoster affecting the lower limbs
Understanding Complex Regional Pain Syndrome
CRPS is a disabling pain condition that typically affects limbs following an injury or surgery. The condition manifests with pain that is disproportionate to the inciting event and is associated with abnormal sensory, motor, sudomotor, vasomotor, and trophic findings.
Classification
CRPS is classified into two types:
- CRPS Type 1 (Reflex Sympathetic Dystrophy): Occurs when there is no obvious nerve injury. This type primarily involves nociceptive pain mechanisms.
- CRPS Type 2 (Causalgia): Occurs when there is an obvious nerve injury. This type involves significant neurogenic components of pain.
In clinical practice, these conditions often present with overlapping symptoms, making clear distinction challenging in some cases.
Clinical Presentation
Patients with CRPS typically present with a constellation of symptoms:
- Severe, burning pain
- Paresthesia (abnormal sensations)
- Edema (swelling)
- Limited range of motion
- Temperature changes in the affected limb
- Skin changes, including color and texture alterations
- Hyperalgesia (increased sensitivity to pain)
- Allodynia (pain from stimuli that are not normally painful)
Pathophysiology
While the definitive pathophysiology of CRPS remains incompletely understood, current evidence suggests it is a disorder of the immune system that affects the nervous system. The condition involves complex interactions between:
- Peripheral and central sensitization
- Neurogenic inflammation
- Autonomic dysregulation
- Immune system activation
- Psychological factors
Diagnosis
Diagnosis of CRPS is primarily clinical, based on established criteria such as the Budapest Criteria, which include:
- Continuing pain disproportionate to any inciting event
- At least one symptom in each of the four categories: sensory, vasomotor, sudomotor/edema, and motor/trophic
- At least one sign at time of evaluation in two or more categories
- No other diagnosis better explaining the signs and symptoms
Case Study: CRPS Following Knee Surgery
Patient Profile
A young male patient was referred to the pain management service from the orthopedic department at Burjeel Day Surgery Center, Al Reem Island. The patient had undergone right knee surgery three months prior and subsequently developed symptoms consistent with CRPS.
Clinical Presentation
Upon evaluation, the patient presented with:
- High skin temperature in the affected limb
- Severe pain (VAS 7/10)
- Mild swelling
- Hypoesthesia (decreased sensation) along the lateral limb
- Allodynia (pain from non-painful stimuli) along the anterior aspect of the limb
- Limited range of motion
Previous Management
The patient had previously received conservative management, including:
- Analgesic medications
- Physical therapy
- Activity modification
Unfortunately, these conventional approaches proved ineffective in providing adequate pain relief or functional improvement.
Intervention Plan
After comprehensive evaluation and proper counseling regarding expectations and potential outcomes, a management plan was formulated:
- Perform a diagnostic lumbar sympathetic block at the right L3 level to assess response
- If favorable response achieved, proceed with radiofrequency ablation for longer-term relief
- Continue multimodal pain management alongside interventional approaches
Procedure Details
Under appropriate monitoring and sterile conditions, a lumbar sympathetic diagnostic block was performed at the right L3 level. Local anesthetic was precisely delivered to the sympathetic chain using fluoroscopic guidance to ensure accurate needle placement.
Outcomes
The results of the intervention were impressive:
- The patient reported being pain-free immediately following the procedure
- Significant improvement in range of motion was observed
- Reduced allodynia in the affected limb
- Normalization of skin temperature
Based on this positive response to the diagnostic block, the patient was scheduled for radiofrequency ablation to provide more sustained relief. The treatment plan continues at Burjeel Day Surgery Center, Al Reem Island.
Discussion
Efficacy of Lumbar Sympathetic Block in CRPS
This case illustrates the potential efficacy of lumbar sympathetic blockade in managing CRPS of the lower extremity. While CRPS is notoriously difficult to treat and often has no definitive cure, timely interventional procedures can:
- Slow disease progression
- Provide crucial pain relief
- Improve function and quality of life
- Help patients cope with daily activities
- Potentially prevent long-term disability
Timing of Intervention
Early intervention is critical in CRPS management. Research suggests that outcomes are generally better when appropriate treatments are initiated within 3-6 months of symptom onset. In this case, the patient was referred approximately three months after surgery, allowing for timely intervention before the condition became more refractory to treatment.
Limitations of Treatment
It’s important to acknowledge certain limitations in CRPS management:
- CRPS typically has no definitive cure
- Treatment responses can be variable
- Multiple interventions may be necessary
- A multimodal approach is often required
Advantages of Lumbar Sympathetic Block
As demonstrated in this case, lumbar sympathetic blockade offers several advantages:
- Minimally Invasive: The procedure requires only needle insertion rather than open surgery
- Diagnostic and Therapeutic: Can serve both to confirm sympathetically maintained pain and provide relief
- Targeted Approach: Directly addresses the sympathetic component of pain
- Low Complication Rate: When performed by experienced practitioners
- Option for Progression: Can progress from diagnostic blocks to more permanent interventions like radiofrequency ablation
Clinical Implications
This case highlights several important clinical implications for pain practitioners:
- Early Recognition: Identifying CRPS early improves outcomes. Healthcare providers should maintain a high index of suspicion for CRPS in patients with disproportionate pain following surgery or injury.
- Prompt Referral: Timely referral to pain specialists when conservative measures fail can prevent progression to chronic, refractory pain states.
- Stepped Approach: A graduated approach from diagnostic blocks to more definitive interventions allows for personalized treatment planning.
- Multimodal Strategy: Even with successful interventional procedures, a comprehensive approach including physical therapy, psychological support, and appropriate medications optimizes outcomes.
Conclusion
Lumbar sympathetic block represents a safe and effective procedure for alleviating pain in patients with CRPS who are refractory to medical management. This case demonstrates the potential for significant improvement in pain and function following appropriate interventional management.
While CRPS remains a challenging condition to treat, a timely, multimodal approach that includes targeted interventions like lumbar sympathetic blockade can significantly improve patient outcomes and quality of life. This case emphasizes the importance of early diagnosis, prompt referral to pain specialists, and individualized treatment planning in the management of complex pain conditions.
For patients suffering from CRPS of the lower extremities who have not responded to conservative management, lumbar sympathetic block should be considered as part of a comprehensive pain management strategy.

