Introduction
Retrocaval ureter, also known as circumcaval ureter, is an exceptionally rare congenital anomaly in which the ureter passes behind the inferior vena cava, creating a potential obstruction to urine flow. With a reported worldwide incidence of only 0.06-0.17% of the population, most medical professionals will never encounter this condition in their career. The anomaly is even more uncommon in children, as most cases are diagnosed in adults during the third or fourth decade of life.
This case study details the successful diagnosis and surgical management of retrocaval ureter in a 15-year-old patient at Burjeel Farha in Al Ain, United Arab Emirates. The case highlights the importance of appropriate diagnostic imaging in children with persistent, unexplained abdominal symptoms and demonstrates how targeted surgical intervention can dramatically improve quality of life for patients with this rare condition.
Understanding Retrocaval Ureter
Embryological Basis
Retrocaval ureter is fundamentally a venous anomaly rather than a ureteral one. During embryological development, the right subcardinal vein normally regresses, and the supracardinal vein forms the infrarenal portion of the inferior vena cava (IVC). In retrocaval ureter, the subcardinal vein persists and forms the infrarenal IVC, causing the ureter to course posterior to it. This creates an S-shaped or reverse J-shaped proximal ureter that winds around the IVC, potentially causing functional obstruction.
Classification
Retrocaval ureters are classified into two types based on radiographic appearance:
- Type I (more common): Shows moderate to severe hydronephrosis with the ureter having an S-shaped or “fishhook” deformity
- Type II (less common): Shows milder hydronephrosis with the ureter having a sickle-shaped curve
Clinical Presentation
The clinical manifestations of retrocaval ureter can vary widely:
- Some patients remain asymptomatic throughout life
- Others develop symptoms in adolescence or adulthood
- Common symptoms include flank pain, recurrent urinary tract infections, hematuria, and renal calculi
- Symptoms are typically related to the degree of ureteral obstruction and subsequent hydronephrosis
Diagnosis is frequently delayed due to the rarity of the condition and the nonspecific nature of symptoms, which may mimic more common disorders like urolithiasis or pyelonephritis.
Case Presentation
Patient History
A 15-year-old male patient presented to Burjeel Farha Hospital in Al Ain for the first time, accompanied by his parents. They reported that their son had been experiencing irregular abdominal pain and vomiting several times per week for several years. Despite consultations with numerous physicians who had suggested allergies and gastric disorders as potential causes, the prescribed medications had provided only temporary relief.
The parents noted a concerning progression in their son’s condition, with worsening pain and daily episodes of vomiting in recent months. This deterioration in his symptoms prompted them to seek further medical evaluation.
Initial Evaluation
The patient was initially assessed by a pediatrician at Burjeel Farha, who ordered an abdominal ultrasound—remarkably, the first ultrasound examination the child had ever undergone despite years of symptoms. The ultrasound revealed significant dilation of the right renal pelvis (hydronephrosis), prompting referral to Dr. Humam Qaraschouli, Consultant Urologist and Head of the Urology Department.
Dr. Qaraschouli performed a repeat ultrasound himself to further evaluate the findings. The examination confirmed hydronephrosis but also showed dilation of the proximal ureter, suggesting that the condition was not a typical ureteropelvic junction obstruction. To rule out urinary calculi as a cause of obstruction, a non-contrast CT scan of the abdomen was ordered. While this study confirmed the absence of stones, it revealed an unusual course of the right ureter.
Definitive Diagnosis
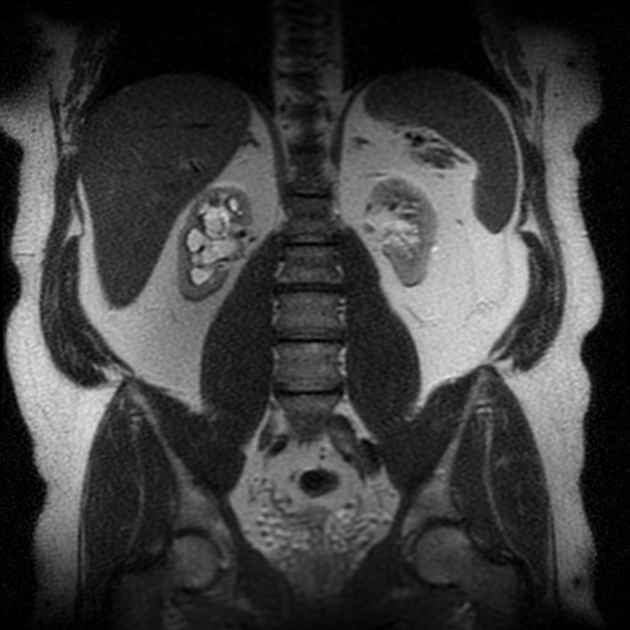
Based on the suspicious findings, a follow-up contrast-enhanced CT scan was performed, which clearly demonstrated the retrocaval course of the right ureter. The imaging showed the classic J-hook or reverse S appearance of the proximal ureter as it traveled behind the inferior vena cava before continuing its normal path to the bladder. The diagnosis of retrocaval ureter was established.
To complete the evaluation and better visualize the distal ureter (which was not clearly visible on the CT scan), a cystoscopy with retrograde ureterography was performed. This confirmed the diagnosis and provided additional anatomical details essential for surgical planning.
Surgical Management
Preoperative Planning
Given the patient’s young age, progressive symptoms, and confirmed anatomical abnormality, surgical correction was deemed necessary. The goals of surgery were to:
- Relieve the obstruction
- Restore normal urinary drainage
- Preserve renal function
- Alleviate the patient’s symptoms
The surgical approach chosen was an open flank incision rather than laparoscopic or robotic techniques, considering the specific anatomical details of this case.
Surgical Procedure
Under general anesthesia administered by Dr. Maitham Badawy, Specialist Anesthesia, Dr. Qaraschouli performed the following steps:
- A right flank incision was made to access the retroperitoneal space
- The right ureter was identified and carefully exposed
- The ureter was divided at the point where it passed behind the inferior vena cava
- The ureter was fully mobilized from its retrocaval position
- The ureter was relocated to its normal anatomical position, anterior to the inferior vena cava
- Spatulation of both cut ends of the ureter was performed to widen the anastomosis
- A double-J ureteral stent was placed to maintain patency during healing
- An end-to-end ureteral anastomosis was performed to reestablish urinary continuity
- The incision was closed in layers
Postoperative Care
Four weeks after the initial procedure, the patient underwent a second brief procedure to remove the double-J stent. At this time, ureteroscopy with ureterography was performed to assess the healed anastomosis and confirm unobstructed urinary flow. The evaluation showed excellent results with a patent ureter and no evidence of stenosis at the anastomotic site.
Clinical Outcome
The results of this intervention were dramatic and immediate. Following surgery, the patient experienced complete resolution of his long-standing symptoms. The abdominal pain and vomiting that had plagued him for years disappeared entirely. At follow-up, he was described as being in “perfect condition,” with a remarkable improvement in his quality of life.
The parents reported their satisfaction with the care provided at Burjeel Farha and expressed gratitude that they did not need to travel abroad for this specialized procedure. This highlights the importance of advanced pediatric urological expertise being available within the region.
Discussion
Clinical Significance
This case underscores several important clinical lessons:
- Importance of Imaging: Despite years of symptoms and multiple medical consultations, this was the first time the patient had undergone ultrasound imaging. Earlier imaging might have led to earlier diagnosis and intervention, potentially preventing years of suffering.
- High Index of Suspicion: The diagnosis of retrocaval ureter requires awareness of this rare entity and appropriate diagnostic workup when hydronephrosis is identified without an obvious cause.
- Value of Comprehensive Evaluation: The stepwise diagnostic approach—from ultrasound to non-contrast CT to contrast-enhanced CT and finally to retrograde ureterography—was essential for accurate diagnosis and surgical planning.
- Effective Surgical Intervention: Despite the rarity of the condition, surgical correction with ureteral reanastomosis proved highly effective, with immediate and complete symptom resolution.
Epidemiological Context
The extreme rarity of this condition cannot be overstated. With a worldwide incidence between 0.06-0.17%, retrocaval ureter is one of the least common congenital urological anomalies. Most reported cases in the literature involve adults, making this pediatric case even more unusual.
The condition shows a male predominance with a male-to-female ratio of approximately 3:1, which aligns with this case of a male patient. This gender disparity is likely related to the embryological development of the inferior vena cava.
Comparison with Alternative Approaches
While this case was managed with traditional open surgery, it’s worth noting that minimally invasive approaches have been described in the literature:
- Laparoscopic Repair: Can be performed with transperitoneal or retroperitoneal approaches, offering benefits of smaller incisions and faster recovery
- Robotic-Assisted Repair: Provides enhanced visualization and precision for the ureteral anastomosis
- Endourological Management: In select cases, ureteral stenting alone may provide symptom relief in patients who are poor surgical candidates
The choice of open surgery in this case was appropriate given the patient’s specific anatomy and the surgeon’s expertise. The excellent outcome validates this approach, though future similar cases might benefit from minimally invasive techniques as expertise with these approaches continues to evolve.
Conclusion
This case represents a successful diagnosis and surgical management of an exceptionally rare congenital anomaly in a pediatric patient. After years of misdiagnosis and ineffective treatments, the patient experienced complete symptom resolution following surgical correction of his retrocaval ureter.
The case highlights several important points for medical practitioners:
- The critical role of appropriate imaging studies in evaluating persistent, unexplained abdominal symptoms in children
- The need to consider rare anatomical anomalies when common diagnoses fail to explain a patient’s symptoms
- The dramatic improvement in quality of life that can result from correct diagnosis and appropriate surgical intervention
For the medical community in the UAE, this case demonstrates the high level of specialized pediatric urological expertise available at Burjeel Farha in Al Ain, eliminating the need for families to travel internationally for complex urological care.
Most importantly, for the young patient in this case, a rare diagnosis followed by expert surgical correction has transformed his life, freeing him from years of unexplained pain and allowing him to enjoy a normal, symptom-free adolescence.

